





SLOAN | Public option palmed off on insurers
We were introduced this week to the forty-somethingth revision to the public health care option bill. This is the latest attempt at conquering once and for all the eternal, seemingly insoluble problem of rising medical costs by reordering the architecture of health care in the state. The fatal flaw of this bill, as all of its previous iterations, is that it reorders health care precisely in the direction of exacerbating the problem.
The original concept of the bill was to establish a state-government run health insurance plan — the Colorado Option Authority — which would have rates artificially set lower than existing market plans; health care providers and insurance companies would then have a couple years to lower their rates accordingly or that option would be unleashed on the industry, and hospitals and doctors would be forced to accept it, on pain of enormous fines and risk of loss of license.
The newest version passed on Tuesday does away with a full-blown state insurance option, and instead has the Department of Insurance conjure up a “standardized plan” which insurance carriers in the small group and individual markets will be required to offer. That plan will be assigned a premium rate that is magically 18% lower, at minimum, than the rates for the plans said insurance carriers offer in 2021.
This “standardized plan” is essentially the public option of yore but instead of the state government running it as a monopoly, it merely tells the insurance companies they have to.
Furthermore, it requires hospitals and providers to accept the cut-rate plan; the fines for not doing so are less than those prescribed in the original bill, but still severe.
Perhaps even more pernicious is the continuation of the theme that has been a troubling constant in the last several years, and that is the dissipation of authority to unelected state bodies. Whereas most of the bills passed by the legislature that serve as a catheter doling out authority to the bureaucracy, gift that power to a group of bureaucrats – a department, agency, or commission — in this case that power is being vouchsafed to a single bureaucrat — the commissioner of insurance.
Those poor souls who are intimately familiar with each of the 17 pages of the new bill inform me that that “commissioner of insurance” is mentioned some 52 times. This individual is granted, among other things, the power to tell insurance carriers what plans to sell — i.e. the standardized plan — what the premium rates for that plan are to be, and what reimbursement rates hospitals and individual health care providers have to pay. It’s a pretty sweet gig if you can get it. Aspiring oligarchs the world over must be taking envious notes.
Now all of this is being done, in fairness, to try and arrest the rising costs of health care. The problem is an entangled one, inasmuch as it admittedly does not yield readily to the usual free market strictures. There are a few reasons for this, but the primary one comes down to the fact that ours is a society that is well consolidated around the idea that no one should die simply because they cannot afford a doctor. We accept that, quite rightly, as axiomatic, implicitly also accepting that that means a certain amount of health care must be subsidized. And the corollary to that is that anything which is subsidized will be over-used, and health care is.
Mark Hillman laid out the problem succinctly the other day in these pages, and that is that none of the measures put in place by governments to artificially reduce the price of health care at the point of service do anything to reduce cost of providing that care. The government, via the commissioner of insurance, can set rates wherever he likes, the cost is going to recovered somewhere, either by someone paying more, or by a reduction in quantity, or an erosion of quality.
This makes it a political question, and right now it is deemed politically expedient to make the hospitals take it on the chin; despite the fact that more than half of hospitals in the state are operating at a financially unsustainable level, with profit margins below 1 percent. But at some point we need to admit that conventional approach to health care reform, i.e. having government absorb more and more of the entire medical enterprise, is making the problem worse, and that what we are really talking about when we talk health care reform is who pays for it and how.
Kelly Sloan is a political and public affairs consultant and a recovering journalist based in Denver.
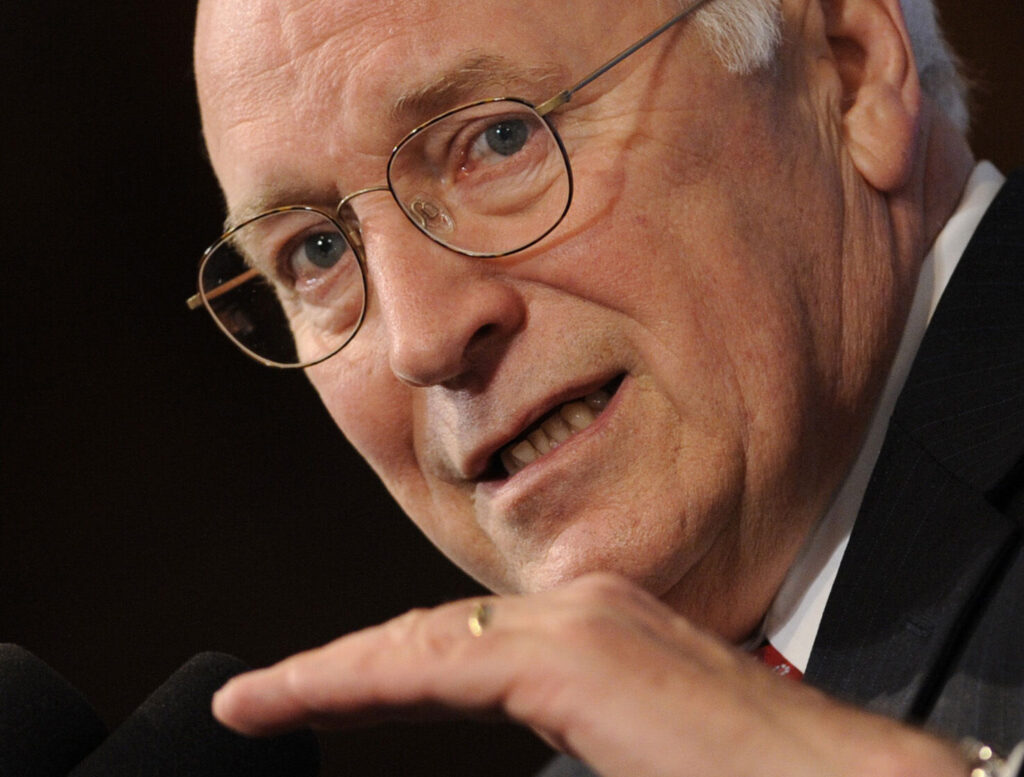
Dick Cheney, one of the most powerful and polarizing vice presidents in US history, dies at 84
Calvin Woodward
calvin-woodward@gazette.com
Updated 5 hours ago
WASHINGTON (AP) — Dick Cheney, the hard-charging conservative who became one of the most powerful and polarizing vice presidents in U.S. history and a leading advocate for the invasion of Iraq, has died at age 84. Cheney died Monday night...
Calvin Woodward
Reporter
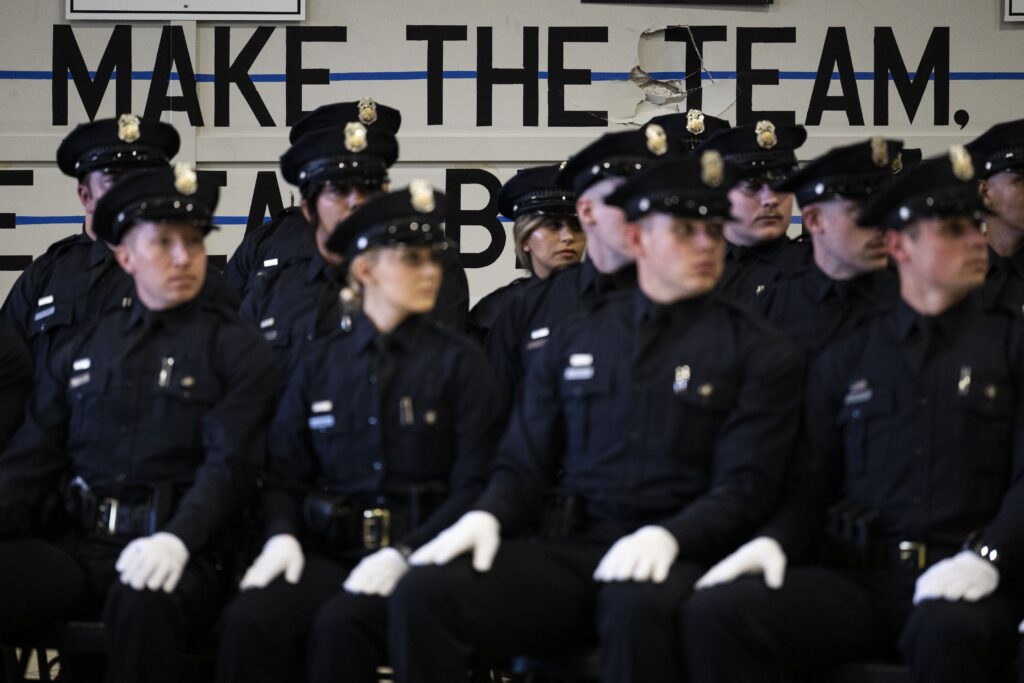
Denver Council rejects push to pull millions from police for homeless spending
Deborah Grigsby
deborah.smith@denvergazette.com
Updated 6 hours ago
A push to shift millions of dollars away from the Denver Police Department to pay for homeless families’ shelter failed on Monday night, when councilmembers waded through more than two dozen amendments. The council voted against a pair of amendments,...
Deborah Grigsby
Reporter

Government shutdown could become longest ever as Trump says he ‘won’t be extorted’ by Democrats
Mary Clare Jalonick
mary.clare.jalonick@associatedpress.com
Updated 1 day ago
WASHINGTON (AP) — The government shutdown is poised to become the longest ever this week as the impasse between Democrats and Republicans has dragged into a new month. Millions of people stand to lose food aid benefits, health care subsidies...
Mary Clare Jalonick
Reporter

Builders say state’s push fails to create more affordable housing
Mark Samuelson
mark-samuelson@denvergazette.com
Updated 53 minutes ago
What’s the secret sauce for making homes more affordable in Colorado? That’s the question that renters are asking when the median price of a home — now $550,000 — ranks Colorado as one of the least affordable places to live...
Mark Samuelson
Reporter

Why do out-of-state donors have more power than in-state voters? | Vince Bzdek
Vince Bzdek
vince-bzdek@denvergazette.com
Updated 1 day ago
Why is Michael Bloomberg, the former presidential candidate, three-term New York mayor and founder of the financial info firm that bears his name, spending millions on Colorado elections? The short answer: because he can. The liberal New Yorker has donated...
Vince Bzdek
Reporter

Denver ramps up efforts to increase affordable housing
Deborah Grigsby
deborah.smith@denvergazette.com
Updated 54 minutes ago
With a population of more than 729,000 and growing, the city of Denver has long struggled with an unaffordable housing market and needs to create close to 44,000 affordable units over the next decade, according to the city’s Department of...
Deborah Grigsby
Reporter

Searching for the ‘missing middle’: Denver metro area cities scramble to meet housing needs
Sage Kelley
sage-kelley@denvergazette.com
Updated 24 hours ago
As Denver and other cities in the metro area race to comply with state mandates to change zoning and plan for more affordable housing, it remains to be seen if their varied approaches will succeed. Laws enacted in 2024 require...
Sage Kelley
Reporter

2 judges order Trump administration to use contingency funds for SNAP payments during the shutdown
Geoff Mulvihill
geoff.mulvihill@associatedpress.com
Updated 3 days ago
BOSTON (AP) — Two federal judges ruled nearly simultaneously on Friday that President Donald Trump’s administration must to continue to fund SNAP, the nation’s biggest food aid program, using contingency funds during the government shutdown. The rulings came a day...
Geoff Mulvihill
Reporter

Gov. Polis proposes privatizing Pinnacol Assurance to address next year’s budget deficit
Marianne Goodland
marianne-goodland@denvergazette.com
Updated 3 days ago
Gov. Jared Polis is hoping for a windfall from the privatization of Colorado’s quasi-public workers’ compensation insurance division to cover some of the anticipated deficits in next year’s operating budget. The 2026-27 state budget, as proposed by the governor, amounts...
Marianne Goodland
Reporter

Gov. Jared Polis abruptly cancels unpublicized meeting with Joint Budget Committee
Marianne Goodland
marianne-goodland@denvergazette.com
Updated 4 days ago
Gov. Jared Polis was scheduled to talk to reporters at 12:30 p.m. on Friday at the Governor’s Mansion to discuss his budget proposal for the upcoming fiscal year, which he is required to submit to the Joint Budget Committee on...
Marianne Goodland
Reporter